
What Guideline I Actually Means in Plain English
Guideline I is the part of the security clearance system that evaluates:
👉 psychological conditions and emotional stability.
In plain English, it asks:
👉 “Does this person’s psychological condition create concern about judgment, reliability, stability, emotional control, or future ability to safeguard classified information?”
That does not mean the government automatically denies clearances to people who:
- attend therapy
- take medication
- experience anxiety or depression
- receive PTSD treatment
- or seek mental-health support
In fact, many cleared professionals—including military personnel, intelligence officers, federal employees, and contractors—successfully maintain security clearances while receiving treatment for psychological conditions.
This is one of the most misunderstood realities in the clearance system.
Guideline I is not really about whether someone has a diagnosis.
It is about whether the overall record suggests:
- impaired judgment
- emotional instability
- poor impulse control
- unpredictability
- behavioral unreliability
- unmanaged psychological risk
- or future inability to function safely in a national-security environment
At its core, Guideline I is a predictability and stability guideline.
The government is evaluating whether psychological conditions appear:
👉 professionally manageable and unlikely to compromise long-term reliability.
That distinction matters enormously.
Many applicants facing Guideline I concerns are not dangerous, unstable, or incapable of performing cleared work.
They are often:
- military veterans with PTSD
- federal employees managing anxiety or depression
- professionals receiving therapy during stressful life events
- applicants taking prescribed medication appropriately
- or individuals who experienced temporary emotional crises years earlier
Common Guideline I issues include:
- PTSD
- anxiety disorders
- depression
- panic attacks
- ADHD and neurodivergence
- hospitalization history
- suicide-related events
- emotional instability under stress
- prescription medication concerns
- counseling or therapy disclosures
- treatment noncompliance
- or psychological evaluations triggered during investigation
At National Security Law Firm, our security clearance lawyers understand that Guideline I cases are often misunderstood because applicants focus on the diagnosis itself instead of how adjudicators actually evaluate risk.
Most adjudicators are not asking:
👉 “Does this applicant have a mental-health history?”
They are usually asking something much more specific:
👉 “Does the overall record suggest stable judgment, emotional predictability, treatment compliance, and future reliability?”
That is the real issue.
Two applicants may both receive therapy for anxiety and receive completely different outcomes.
One applicant may:
- engage responsibly in treatment
- comply with medication
- maintain strong professional functioning
- demonstrate years of stability
- and present a calm, medically supported record
Another may:
- abruptly stop treatment
- conceal counseling
- minimize obvious instability
- become emotionally reactive during investigation
- or create contradictory psychological records
Those are not the same security-clearance file.
In Guideline I cases, the issue is not simply:
👉 whether someone sought help.
The issue is:
👉 what the overall record suggests about future reliability, emotional stability, predictability, and ability to function safely over time.
Quick Answer: Can Mental Health Affect Your Security Clearance?
Yes.
Psychological conditions and emotional-stability concerns can affect security clearance eligibility.
Guideline I concerns can result in:
- clearance delay
- additional investigation
- psychological evaluation requests
- a Letter of Interrogatory (LOI)
- a Statement of Reasons (SOR)
- suspension
- denial
- or revocation
Common Guideline I issues include:
- PTSD
- anxiety
- depression
- hospitalization history
- emotional instability
- panic attacks
- suicide-related events
- medication concerns
- counseling disclosures
- treatment noncompliance
- or behavior suggesting impaired judgment or unpredictability
But this is the critical point:
👉 treatment itself is often NOT the problem.
Many applicants with:
- PTSD
- anxiety
- depression
- ADHD
- or prior counseling history
still maintain or obtain clearances successfully.
The issue is usually not:
👉 whether someone received treatment.
The issue is:
👉 whether the overall record creates unresolved concern about future judgment, reliability, emotional control, or predictability.
That is where cases become dangerous.
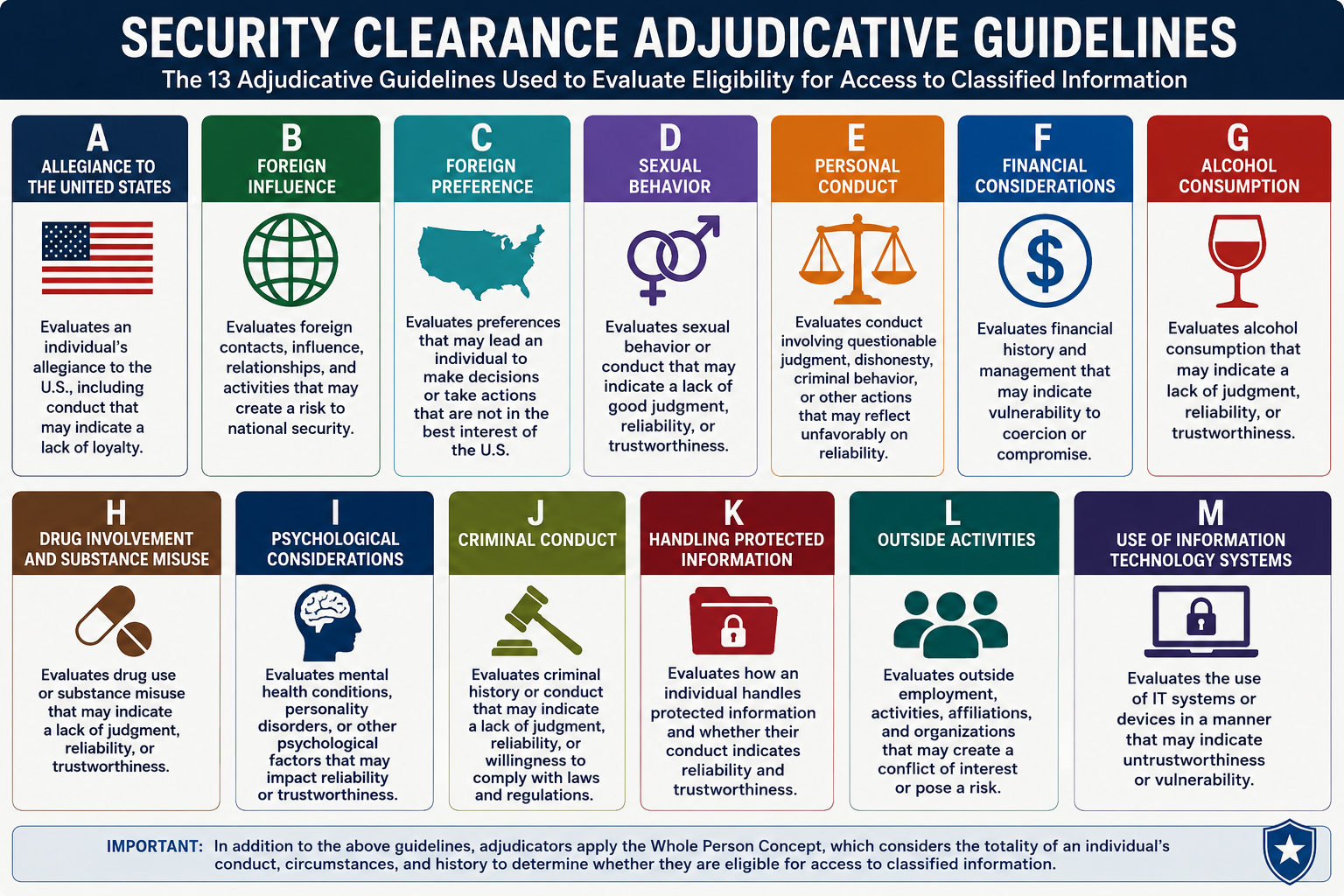
To understand how Guideline I fits into the broader clearance decision framework, review the:
👉 Security Clearance Adjudicative Guidelines
Why Guideline I Is One of the Most Misunderstood Guidelines
Few guidelines generate more confusion than Guideline I.
Applicants often assume:
- therapy hurts clearances
- counseling creates permanent risk
- medication makes them look unstable
- PTSD automatically disqualifies military personnel
- or hospitalization permanently destroys eligibility
Those assumptions are often wrong.
In reality, modern security-clearance adjudication usually focuses much more heavily on:
- treatment compliance
- emotional stability
- behavioral predictability
- professional functioning
- and whether future risk appears manageable
This is one reason many applicants unintentionally make their cases worse.
They panic.
They:
- stop therapy
- discontinue medication abruptly
- hide counseling history
- avoid evaluations
- or become emotionally defensive during the process
Ironically, those reactions often create more adjudicative concern than the underlying condition itself.
This is one of the most important realities of Guideline I:
👉 untreated or unmanaged instability is often viewed as far more dangerous than responsible treatment and documented recovery.
For example:
An applicant attending therapy consistently, maintaining stable employment, complying with treatment, and functioning successfully for years may appear significantly less risky than:
👉 an applicant with no formal diagnosis whose behavior appears impulsive, unstable, unpredictable, or emotionally unmanaged.
That distinction matters enormously.
Adjudicators are usually not trying to identify people who have never struggled emotionally.
They are trying to determine:
👉 whether the applicant appears stable, predictable, professionally manageable, and safe to trust long-term with classified access.
Why Guideline I Cases Feel So Personal
Guideline I cases feel different from many other security-clearance issues.
A financial problem may feel stressful.
A foreign-contact issue may feel complicated.
A drug issue may feel embarrassing.
But psychological-condition concerns often feel:
👉 deeply personal.
Applicants frequently feel like the government is questioning:
- their emotional stability
- their judgment
- their reliability
- or even their identity
This creates a very different emotional reaction than most other adjudicative guidelines.
Many applicants immediately begin thinking:
- “They think I’m unstable.”
- “They think I can’t handle pressure.”
- “They think therapy means I’m weak.”
- “My career is over because I sought help.”
- “I should never have disclosed counseling.”
- “I shouldn’t have taken medication.”
That fear often becomes the beginning of the real problem.
Because panic causes applicants to:
- conceal treatment
- stop medication suddenly
- emotionally over-explain
- become defensive during evaluations
- or try to “look stronger” than the record realistically supports
Those reactions can quietly damage a case.
Not because adjudicators are punishing treatment.
But because adjudicators are evaluating something else entirely:
👉 whether the applicant appears emotionally predictable and professionally manageable under stress.
This distinction matters enormously.
A person responsibly managing anxiety through therapy may appear far safer than:
👉 someone trying desperately to hide instability while the record quietly deteriorates underneath them.
Guideline I cases are often won or lost based on:
👉 how stable the overall record feels over time.
Not whether emotional difficulty ever existed.
Why the Insider Perspective Matters in Psychological Cases
Most online discussions about Guideline I focus on:
- therapy disclosures
- PTSD
- medication
- or whether a diagnosis is “disqualifying”
That is not enough.
The harder question is:
👉 How do adjudicators actually decide whether a psychological condition creates future security concern?
That is where insider perspective matters.
At National Security Law Firm, we approach Guideline I cases from the perspective of the decision-maker.
Our attorneys understand how adjudicators evaluate:
- emotional stability
- treatment compliance
- hospitalization history
- psychological evaluations
- medication management
- crisis history
- professional functioning
- predictability under stress
- and long-term reliability
For example, adjudicators may ask:
- Is treatment stable and consistent?
- Does the applicant function reliably professionally?
- Are emotional episodes isolated or recurring?
- Is the applicant cooperative with treatment?
- Does the file feel medically supported and predictable?
- Does the applicant appear emotionally reactive or behaviorally unstable?
- Would another crisis appear likely in the future?
- Can approval be defended if the file is reviewed later?
That last question matters enormously.
Because security-clearance adjudication is not simply about diagnosis.
It is about:
👉 whether the government feels comfortable continuing to trust the applicant in sensitive environments over time.
This is why Guideline I cases are often won or lost on:
👉 stability, predictability, treatment compliance, emotional control, and disciplined record management.
Not just the existence of counseling or diagnosis itself.
What This Guide Will Help You Understand
If you are dealing with a Guideline I concern—or worried that one may arise—this guide will explain:
- what psychological conditions actually mean in clearance law
- how therapy and counseling are evaluated
- when PTSD, anxiety, and depression become clearance concerns
- how medication affects adjudicative analysis
- why hospitalization and crisis events are evaluated differently than most applicants assume
- how psychological evaluations influence clearance decisions
- when emotional instability becomes dangerous
- what mitigation actually works
- where applicants accidentally weaken their cases
- and how successful Guideline I cases are built around stability, treatment compliance, and future reliability
Most importantly, this guide will help you understand how the government evaluates psychological conditions from a national-security perspective.
Because until you understand that:
👉 you may be trying to defend treatment while the government is evaluating long-term predictability and professional stability.
That mismatch is where many Guideline I cases begin to fail.
When Guideline I Actually Comes Up in Real Cases
Guideline I concerns usually arise when the government believes:
👉 emotional or psychological conditions may affect judgment, reliability, stability, or future ability to safeguard classified information.
Sometimes the issue involves obvious serious instability.
More often, the issue begins with:
- therapy disclosures
- PTSD treatment
- hospitalization history
- medication use
- emotional crises
- counseling records
- psychological evaluations
- or behavioral concerns raised during investigation
That is why many applicants are surprised when Guideline I appears.
They often think:
👉 “I was responsible enough to seek help.”
Or:
👉 “My condition is fully managed.”
Those things may absolutely help mitigation.
But adjudicators are evaluating something more specific:
👉 whether the overall record still creates unresolved concern about future reliability or predictability.
Below are some of the most common ways Guideline I appears in real security-clearance cases.
Therapy and Counseling
Therapy itself is not automatically disqualifying.
In many cases, therapy actually becomes:
👉 evidence of responsibility and insight.
But counseling can still become part of the adjudicative record where applicants:
- fail to disclose treatment properly
- create inconsistent disclosures
- abruptly stop treatment
- or demonstrate instability despite treatment
The issue is often not:
👉 whether therapy occurred.
It is:
👉 whether the overall record appears stable and professionally manageable.
PTSD
PTSD is one of the most common Guideline I issues involving:
- military veterans
- intelligence personnel
- federal law enforcement
- and applicants exposed to trauma or operational stress
Many applicants incorrectly assume:
👉 PTSD automatically destroys clearance eligibility.
That is usually not true.
Adjudicators frequently evaluate:
- treatment compliance
- emotional control
- professional functioning
- and whether symptoms appear stable and manageable over time
This is one reason many applicants with PTSD successfully maintain clearances when:
- treatment remains stable
- functioning remains reliable
- and the record supports long-term predictability.
Anxiety and Panic Disorders
Anxiety-related conditions appear frequently in security-clearance cases.
Especially among applicants working in:
- high-pressure environments
- intelligence roles
- military operations
- cybersecurity
- aviation
- or mission-critical federal positions
Applicants often panic because they assume:
👉 “Anxiety means I look unstable.”
That is not usually how adjudicators evaluate these cases.
Many applicants with anxiety maintain clearances successfully.
What adjudicators often focus on instead is:
- whether treatment is effective
- whether panic symptoms impair functioning
- whether emotional control appears stable
- and whether the applicant continues functioning reliably under stress
This is one reason treatment compliance and long-term functionality matter so much in anxiety-related Guideline I cases.
Depression
Depression-related concerns are highly fact-specific.
Many applicants fear that:
👉 any history of depression automatically creates clearance risk.
That is not accurate.
Adjudicators often evaluate:
- severity
- treatment history
- current stability
- medication compliance
- and whether the condition affects judgment or reliability
The issue is often not:
👉 whether depression ever existed.
The issue is:
👉 whether the condition now appears stable, treated, and unlikely to impair future functioning.
Applicants who demonstrate:
- long-term treatment compliance
- stable employment
- reliable functioning
- and no recurring crises
often present much stronger mitigation.
ADHD and Neurodivergence
ADHD and neurodivergence are increasingly common issues in modern clearance cases.
Especially where applicants use:
- stimulant medication
- executive-function support
- or ongoing treatment management
Most ADHD-related cases are not fundamentally about the diagnosis itself.
Adjudicators often evaluate:
- whether medication is managed responsibly
- whether functioning remains stable
- whether impulsivity appears controlled
- and whether treatment compliance exists
This becomes more complicated where:
- medication misuse allegations arise
- prescriptions are inconsistent
- or behavioral-control concerns overlap with other guidelines
But many applicants with ADHD maintain clearances successfully without major difficulty.
Prescription Medication Concerns
Prescription medication issues can become part of Guideline I analysis where adjudicators believe:
👉 medication may affect judgment, emotional stability, or reliability.
This is especially important involving:
- anti-anxiety medication
- antidepressants
- sleep medication
- stimulants
- mood stabilizers
- or combinations of psychiatric medication
But adjudicators are often evaluating something more nuanced than applicants realize.
They are asking:
👉 does the treatment appear stable and medically managed?
Or:
👉 does the record feel unpredictable or behaviorally unstable?
This distinction matters enormously.
Medication itself is often far less concerning than:
- misuse
- abrupt discontinuation
- inconsistent compliance
- or unmanaged symptoms afterward
For deeper analysis, review:
👉 Can Prescription Drugs Affect a Security Clearance?
Hospitalization and Crisis Events
Hospitalization-related events create enormous fear in clearance cases.
Applicants often assume:
👉 “A hospitalization automatically ends my career.”
That is not necessarily true.
Many hospitalization-related cases are highly dependent on:
- recency
- recovery
- treatment compliance
- current functioning
- and whether the event appears isolated or predictive of future instability
Adjudicators frequently distinguish between:
👉 temporary crisis
and
👉 ongoing unmanaged instability.
For example:
An isolated emotional crisis years earlier followed by stable treatment and strong professional functioning may appear very different than:
👉 repeated emotional episodes with poor treatment compliance afterward.
The issue is usually not only:
👉 what happened during the crisis.
It is:
👉 what the record suggests about future predictability now.
Suicide Attempts or Self-Harm History
These are among the most emotionally sensitive Guideline I issues.
Applicants often fear:
👉 any suicide-related history permanently destroys eligibility.
That is not necessarily true.
Adjudicators often evaluate:
- how long ago the event occurred
- treatment afterward
- current emotional stability
- relapse risk
- support systems
- and whether the applicant now appears psychologically reliable and professionally functional
This is one reason long-term recovery documentation can become extremely important.
Especially where applicants demonstrate:
- treatment compliance
- emotional stabilization
- professional success
- and absence of recurring crises afterward
Emotional Instability and Behavioral Concerns
Some Guideline I cases are not driven by formal diagnosis at all.
Instead, the concern arises because behavior itself appears:
- emotionally unstable
- impulsive
- unpredictable
- reactive
- or professionally difficult to manage
Examples may include:
- emotional outbursts
- erratic communication
- severe stress reactions
- impulsive conduct
- or unstable workplace behavior
This is one reason adjudicators often care less about labels and more about:
👉 observable reliability over time.
Psychological Evaluations
Psychological evaluations can become central evidence in Guideline I cases.
Especially where adjudicators are trying to determine:
- future risk
- treatment stability
- emotional predictability
- or professional functionality
Strong evaluations often help establish:
- stability
- low future risk
- treatment success
- and reliable functioning
Weak evaluations often create concern where they suggest:
- untreated instability
- poor insight
- emotional volatility
- or unresolved future impairment
This is one reason evaluation strategy matters enormously in Guideline I cases.
Treatment Noncompliance
Treatment noncompliance often creates much greater concern than treatment itself.
Examples include:
- stopping medication abruptly
- refusing counseling
- ignoring medical recommendations
- inconsistent treatment participation
- or abandoning recovery plans without medical support
Adjudicators may interpret these patterns as:
👉 evidence of future instability or poor judgment.
This is one reason many successful Guideline I cases focus heavily on:
👉 consistent treatment management and long-term behavioral stability.
Polygraph and Disclosure Issues
Some Guideline I concerns emerge during:
👉 subject interviews or polygraph examinations.
Applicants sometimes:
- disclose prior hospitalization
- reveal emotional crises
- admit treatment inconsistencies
- or create contradictory mental-health disclosures under stress
Those admissions often become:
👉 permanent parts of the investigative record.
And once multiple explanations begin appearing:
👉 credibility concern can quietly expand the case far beyond the original condition itself.
The Guideline I Statute (Full Text)
The full statutory language for Guideline I can be reviewed here:
👉 § 147.11 Guideline I — Emotional, Mental, and Personality Disorders
The regulation explains:
- what psychological conditions may raise concern
- how adjudicators evaluate emotional stability and reliability
- and what mitigating conditions may apply
But reading the statute alone is not enough.
Because Guideline I cases are rarely decided based solely on:
👉 whether someone received treatment or diagnosis.
They are decided based on:
- stability
- predictability
- treatment compliance
- behavioral functioning
- emotional control
- and whether adjudicators believe future reliability concerns remain unresolved
That is why two applicants with similar diagnoses may receive completely different outcomes.
👉 The difference is often not the diagnosis itself.
👉 It is how the condition appears throughout the broader record over time.
What the Government Is Actually Worried About
To truly understand Guideline I, you have to understand the government’s core concern.
The government is not trying to identify applicants who have never experienced emotional difficulty.
It is evaluating:
👉 whether psychological conditions create future security risk.
That concern generally falls into several categories.
1. Impaired Judgment
This is one of the core Guideline I concerns.
Adjudicators worry that psychological instability may affect:
- decision-making
- impulse control
- emotional regulation
- or professional judgment under stress
This is one reason unmanaged crises or severe emotional instability create heightened concern.
2. Predictability and Stability
Guideline I heavily evaluates:
👉 predictability over time.
Adjudicators often ask:
- Does the applicant appear emotionally stable?
- Does the treatment appear effective?
- Does the file feel professionally manageable?
- Does future functioning appear reliable?
The issue is often not emotional difficulty itself.
It is:
👉 whether future instability appears difficult to predict or control.
3. Behavioral Reliability
Adjudicators also evaluate whether psychological conditions appear connected to:
- impulsive behavior
- emotional volatility
- workplace instability
- impaired functioning
- or poor behavioral control
The concern is usually not treatment.
It is:
👉 whether behavior appears consistently reliable over time.
4. Future Functioning Under Stress
Security-clearance holders often work in:
- stressful
- operational
- classified
- or high-consequence environments
Adjudicators therefore evaluate whether the applicant appears capable of:
👉 functioning safely and reliably under future stress.
This becomes especially important in cases involving:
- crisis history
- emotional breakdowns
- repeated instability
- or untreated conditions
5. Concealment and Credibility Problems
Once psychological-condition concerns become:
- concealed
- minimized
- inconsistently explained
- or emotionally distorted
the case often becomes much more serious.
This is where Guideline I frequently overlaps with:
👉 Guideline E — Personal Conduct
Many otherwise manageable cases become dangerous because:
👉 credibility deterioration becomes more concerning than the treatment history itself.
How Adjudicators Actually Evaluate Guideline I Cases
This is where insider perspective matters most.
Adjudicators do not evaluate Guideline I mechanically.
They do not simply ask:
👉 “Does this person have a psychological condition?”
They ask:
👉 “What does the overall record suggest about future reliability, emotional predictability, judgment, and ability to function safely in a national-security environment?”
That distinction is critical.
Because many Guideline I cases are not really about diagnosis itself.
They are about:
👉 whether the condition appears professionally manageable and unlikely to impair future reliability.
Adjudicators often evaluate several core questions.
Is the Condition Stable and Managed?
This is one of the most important issues in Guideline I.
Adjudicators often evaluate:
- whether treatment appears effective
- whether symptoms remain controlled
- whether functioning appears stable
- and whether emotional predictability improved over time
A treated, stable condition may appear very different than:
👉 unmanaged or escalating instability.
Is Treatment Being Followed Responsibly?
Treatment compliance matters enormously.
Adjudicators often evaluate:
- medication compliance
- counseling participation
- therapy consistency
- psychiatric follow-up
- and whether recommendations are followed appropriately
The issue is often not treatment itself.
It is:
👉 whether the applicant appears responsible and stable while managing the condition.
Has the Applicant Demonstrated Long-Term Reliability?
Time matters heavily in Guideline I.
Applicants who demonstrate:
- stable employment
- strong evaluations
- no recurring crises
- and predictable behavior over long periods
often present much stronger mitigation.
Because adjudicators frequently distinguish between:
👉 temporary emotional difficulty
and
👉 unresolved long-term instability.
Was There Hospitalization or Severe Crisis History?
Hospitalization and crisis events often receive heightened scrutiny.
Especially where records suggest:
- impaired functioning
- suicidal ideation
- self-harm
- severe instability
- or dangerous behavior
But adjudicators also heavily evaluate:
- recovery afterward
- treatment compliance
- current stability
- and long-term functioning
This is one reason many hospitalization-related cases remain highly mitigable.
Does the Record Feel Predictable or Unpredictable?
This is one of the most important insider concepts in Guideline I.
Adjudicators constantly evaluate:
👉 whether the file feels stable enough to approve safely.
If the record feels:
- medically supported
- behaviorally controlled
- emotionally stable
- and professionally manageable
approval becomes much easier to defend.
But if the file feels:
- contradictory
- emotionally volatile
- unmanaged
- or unpredictable
approval becomes much harder.
Did the Applicant React Responsibly to the Issue?
Adjudicators frequently evaluate how applicants responded once concerns emerged.
Applicants who:
- sought treatment
- stabilized behavior
- followed recommendations
- and maintained reliable functioning
often perform far better than applicants who:
- denied obvious instability
- stopped treatment abruptly
- concealed records
- or became emotionally defensive throughout the process
The response to the issue often becomes:
👉 as important as the issue itself.
Can Approval Be Defended?
This is one of the most important insider concepts in clearance law.
Adjudicators constantly ask themselves:
👉 “Could I defend approving this applicant later if another emotional or psychological event occurred?”
That question drives many Guideline I outcomes.
If the file feels:
- stable
- medically supported
- professionally manageable
- and behaviorally predictable
approval becomes much more likely.
If the record feels:
- unstable
- contradictory
- emotionally reactive
- or difficult to assess confidently
approval becomes much harder.
Why Therapy Usually Does NOT Hurt Clearance Cases
This is one of the biggest myths in the entire security-clearance system.
Applicants constantly fear:
👉 “If I go to therapy, I’ll lose my clearance.”
That fear quietly causes enormous damage.
Because many applicants then:
- avoid counseling they genuinely need
- stop treatment abruptly
- conceal therapy history
- avoid medication
- or refuse evaluations entirely
And those decisions often create far more adjudicative concern than therapy itself.
This is one of the most misunderstood realities of Guideline I:
👉 responsible treatment is often viewed much more favorably than untreated instability.
Adjudicators are not looking for applicants who have never experienced:
- stress
- trauma
- grief
- burnout
- anxiety
- depression
- or emotional difficulty
That would not reflect reality inside:
- military service
- intelligence work
- federal law enforcement
- cybersecurity
- aviation
- or high-pressure national-security careers
What often matters much more is:
👉 whether the applicant responded responsibly when those issues arose.
This is why therapy frequently becomes:
👉 evidence of insight, accountability, and emotional self-management.
Especially where treatment appears:
- voluntary
- stable
- effective
- and professionally appropriate
Applicants often imagine adjudicators viewing therapy as evidence of weakness.
In reality, many adjudicators become far more concerned when applicants:
- refuse treatment
- abruptly stop medication
- conceal counseling
- or insist obvious instability never existed
Because those reactions can make the file feel:
👉 unmanaged and unpredictable.
This distinction changes many Guideline I cases completely.
The strongest records often show:
👉 stable treatment, insight, and long-term professional functioning—not emotional perfection.
PTSD, Anxiety, and Depression in Clearance Cases
Conditions like:
- PTSD
- anxiety
- depression
- panic disorder
- trauma-related symptoms
- and stress-related conditions
appear frequently in modern security-clearance cases.
Especially among:
- military personnel
- intelligence professionals
- law-enforcement officers
- federal employees
- and applicants exposed to prolonged operational stress
Many applicants incorrectly assume:
👉 diagnosis alone destroys eligibility.
That is usually not true.
Adjudicators often focus much more heavily on:
- treatment compliance
- current functioning
- behavioral stability
- emotional predictability
- and whether future impairment appears manageable
For example:
An applicant receiving consistent PTSD treatment while maintaining:
- stable employment
- leadership responsibilities
- strong evaluations
- and predictable functioning
may appear significantly less concerning than:
👉 an untreated applicant whose behavior appears emotionally volatile or unstable despite having no formal diagnosis at all.
That distinction matters enormously.
Guideline I is not fundamentally a diagnosis-based system.
It is:
👉 a future-risk and reliability system.
This is why many applicants with:
- PTSD
- anxiety
- depression
- or trauma history
continue holding security clearances successfully.
Especially where the record demonstrates:
- treatment stability
- insight
- long-term functionality
- and emotional predictability over time
Medication and Security Clearance Risk
Medication-related concerns are often misunderstood.
Applicants frequently panic because they believe:
👉 taking psychiatric medication automatically creates clearance danger.
That is usually not how adjudicators evaluate these cases.
The issue is rarely:
👉 “Does this applicant take medication?”
The issue is more often:
👉 “Does the overall record suggest stable functioning while treatment is being managed appropriately?”
Adjudicators frequently evaluate:
- whether medication is taken as prescribed
- whether treatment appears effective
- whether side effects impair functioning
- whether misuse concerns exist
- and whether emotional stability improved over time
This is especially important involving:
- antidepressants
- anti-anxiety medications
- ADHD medication
- mood stabilizers
- sleep medication
- or combinations of psychiatric prescriptions
Medication itself often becomes far less concerning than:
- misuse
- abrupt discontinuation
- inconsistent compliance
- or unmanaged symptoms afterward
This is one reason applicants who responsibly manage medication frequently perform much better than applicants who:
👉 stop treatment suddenly in an attempt to “look healthier” for clearance purposes.
For deeper analysis, review:
👉 Can Prescription Drugs Affect a Security Clearance?
Hospitalization and Crisis Events
Hospitalization-related events create enormous fear in security-clearance cases.
Applicants often assume:
👉 “A hospitalization permanently destroys my eligibility.”
That is not necessarily true.
Many hospitalization-related cases are highly dependent on:
- how long ago the event occurred
- whether treatment was followed afterward
- whether emotional stability returned
- whether additional crises occurred
- and whether current functioning appears reliable and predictable
Adjudicators frequently distinguish between:
👉 temporary crisis
and
👉 unresolved long-term instability.
For example:
A single emotional breakdown during an extreme life event followed by:
- therapy
- recovery
- stable treatment
- and years of reliable functioning
may appear very different than:
👉 repeated crises combined with treatment refusal or escalating instability.
This is one reason many applicants with prior hospitalization still successfully maintain or regain clearances.
The issue is often not:
👉 what happened during the crisis itself.
It is:
👉 what the overall record suggests about future reliability now.
The “Paper Risk” Problem in Guideline I Cases
This is one of the most important concepts in psychological-condition clearance law.
Even manageable emotional conditions can become dangerous when:
👉 the file itself begins to feel unpredictable, contradictory, or emotionally unstable.
This is what we call:
👉 paper risk.
Examples include:
- contradictory evaluations
- emotionally reactive written statements
- unsupported self-assessment
- abrupt treatment changes
- inconsistent disclosures
- unstable medication history
- or records suggesting unmanaged emotional volatility
Once the file begins to feel:
- unpredictable
- emotionally unstable
- professionally difficult to assess
- or medically unsupported
👉 adjudicators become uncomfortable approving it.
That discomfort matters enormously.
Because adjudicators constantly ask themselves:
👉 “Can I defend approving this applicant later if another emotional crisis occurs?”
If the answer becomes uncertain:
👉 the case becomes much harder to win.
This is one reason calm communication, medically supported records, stable treatment history, and disciplined narrative control matter so much in Guideline I cases.
What Strong Guideline I Mitigation Actually Looks Like
Strong Guideline I mitigation is rarely built around proving:
👉 “Nothing was wrong.”
That approach often backfires.
The strongest cases usually focus on something much more persuasive:
👉 demonstrating stability, treatment compliance, emotional predictability, and reliable functioning over time.
Strong mitigation often includes:
- consistent treatment participation
- medication compliance where appropriate
- stable employment and functioning
- strong psychological evaluations
- no recurring crises
- responsible behavioral management
- and credible medical documentation supporting future reliability
The issue is not emotional perfection.
It is:
👉 whether the applicant now appears safe, stable, and professionally manageable long-term.
For a deeper breakdown of what actually helps—and hurts—Guideline I cases, including therapy, medication, hospitalization, evaluations, and psychological-risk mitigation strategy, review:
👉 How to Mitigate a Guideline I Psychological Conditions Security Clearance Concern
What Weak Guideline I Mitigation Looks Like
Weak Guideline I mitigation usually shares one common theme:
👉 the record begins feeling emotionally unmanaged instead of professionally stable.
Applicants often weaken their cases by:
- stopping treatment suddenly
- concealing therapy
- refusing evaluations
- minimizing obvious instability
- emotionally over-explaining
- submitting reactive written responses
- or insisting no issue ever existed despite contradictory records
Those reactions often create far more adjudicative concern than treatment itself.
This is one of the most important realities of Guideline I:
👉 adjudicators are often evaluating management of the condition—not simply the condition itself.
Emotional Defensiveness Quietly Damages Many Guideline I Cases
Applicants frequently react emotionally because Guideline I feels deeply personal.
That reaction is understandable.
But it can quietly damage the file.
Especially where applicants begin:
- arguing emotionally with evaluators
- repeatedly rewriting explanations
- attacking treatment recommendations
- or attempting to prove they are “fine” through increasingly unstable communication
Adjudicators often interpret these patterns differently than applicants expect.
Instead of seeing strength, they may begin seeing:
👉 instability under stress.
This is one reason calmness, discipline, and professional communication matter so much in Guideline I cases.
Abrupt Treatment Changes Create Major Problems
Applicants sometimes stop:
- therapy
- counseling
- medication
- or psychiatric follow-up
because they fear treatment itself creates clearance risk.
That strategy often backfires badly.
Because adjudicators may now begin worrying that:
👉 the applicant is avoiding responsible management of the condition.
In many situations, treatment compliance actually strengthens mitigation substantially.
Especially where treatment appears:
- stable
- medically supervised
- and professionally effective
Unsupported Self-Assessment Is Often Dangerous
Applicants frequently say things like:
- “I’m completely fine now.”
- “I don’t need treatment anymore.”
- “The evaluator exaggerated.”
- “There was never really a problem.”
Those statements sometimes weaken cases when:
👉 the record suggests otherwise.
Adjudicators often place much greater weight on:
- documented treatment history
- professional evaluations
- counseling records
- and long-term behavioral evidence
than unsupported personal conclusions alone.
This is one reason professionally supported mitigation matters so much.
Illustrative Guideline I Case Scenarios
The examples below are hypothetical scenarios based on common fact patterns seen in security-clearance cases. They are designed to show how adjudicators typically evaluate Guideline I concerns—not to predict outcomes in any specific case.
Scenario 1 — PTSD Treatment With Stable Functioning (Often Mitigable)
A military applicant receives treatment for PTSD after deployment.
The applicant:
- complies with counseling
- follows treatment recommendations
- maintains stable employment
- and demonstrates no behavioral instability afterward
👉 Likely Outcome: Often mitigable
Why this works:
The record supports stability, insight, and responsible treatment management.
Scenario 2 — Anxiety Treated Successfully While Maintaining Clearance (Often Manageable)
An applicant receives treatment for anxiety but continues functioning successfully in a cleared position.
👉 Likely Outcome: Often manageable
Why this works:
Treatment itself does not automatically create adjudicative concern where functioning remains stable.
Scenario 3 — Abruptly Stopping Medication Without Guidance (Higher Risk)
An applicant suddenly stops medication because they fear treatment records will hurt clearance eligibility.
The applicant later experiences instability.
👉 Likely Outcome: Elevated concern
Why this creates concern:
The unmanaged treatment change creates greater risk than the medication itself.
Scenario 4 — Hospitalization Years Earlier Followed by Long-Term Recovery (Potentially Mitigable)
An applicant experienced a psychological crisis and hospitalization many years earlier but has maintained stable treatment and professional functioning ever since.
👉 Likely Outcome: Often manageable
Why this works:
The event appears historical rather than predictive of ongoing instability.
Scenario 5 — Refusal to Participate in Evaluation (High Risk)
An applicant refuses psychological evaluation while simultaneously minimizing obvious instability concerns.
👉 Likely Outcome: Significant Guideline I concern
Why this fails:
The refusal creates concern about insight, cooperation, and future predictability.
Scenario 6 — ADHD Medication With Stable Compliance (Often Mitigable)
An applicant takes ADHD medication under consistent medical supervision and demonstrates stable functioning.
👉 Likely Outcome: Often manageable
Why this works:
Medication alone rarely creates concern where treatment remains stable and compliant.
Scenario 7 — Emotional Overreaction During Investigation (Higher Risk)
An applicant submits emotionally reactive written responses and repeatedly changes explanations during the process.
👉 Likely Outcome: Elevated concern
Why this creates concern:
The record begins feeling unstable and difficult to assess predictably.
Scenario 8 — Depression Treated Successfully With Long-Term Stability (Strong Mitigation)
An applicant receives treatment for depression, follows recommendations, maintains stable employment, and demonstrates years of reliable functioning afterward.
👉 Likely Outcome: Strong mitigation
Why this helps:
The record supports predictability, recovery, and professional reliability.
Scenario 9 — Untreated Emotional Instability With Escalating Conduct (High Risk)
An applicant refuses treatment while demonstrating escalating emotional and behavioral instability.
👉 Likely Outcome: Severe Guideline I concern
Why this fails:
The record suggests unresolved future reliability risk.
Scenario 10 — Therapy During Divorce or Personal Crisis (Often Mitigable)
An applicant seeks counseling during a divorce and temporary emotional crisis but stabilizes afterward without recurring problems.
👉 Likely Outcome: Often manageable
Why this works:
The treatment reflects responsible management of temporary stress rather than long-term instability.
What Actually Gets Guideline I Cases Approved
Successful Guideline I cases usually share several characteristics.
The applicant typically:
- demonstrates emotional and behavioral stability
- complies with treatment recommendations
- maintains credible medical support
- functions reliably in professional settings
- avoids recurring crises
- and presents a record that feels predictable and professionally manageable over time
Most importantly:
👉 the adjudicator ultimately believes the applicant’s condition no longer creates meaningful future security risk.
That is the real issue in Guideline I.
Not perfection.
👉 long-term reliability, predictability, and stability.
What Causes Guideline I Denials
Guideline I denials usually stem from one core conclusion:
👉 the adjudicator believes future instability or impairment risk remains unresolved.
That concern may involve:
- untreated instability
- refusal of treatment
- repeated emotional crises
- unmanaged symptoms
- contradictory evaluations
- medication noncompliance
- dishonesty
- unpredictable behavior
- or inability to function reliably in sensitive environments
This is one of the most important realities of Guideline I:
👉 denials often occur because adjudicators believe the future risk remains difficult to predict—not simply because a diagnosis exists.
Where Guideline I Cases Collapse
Most Guideline I cases do not fail because someone attended therapy or received treatment.
They fail during escalation.
This is one of the most important concepts in psychological-condition clearance law.
Stage 1 — Emotional or Psychological Difficulty Emerges
Examples include:
- PTSD symptoms
- anxiety
- depression
- trauma-related stress
- panic episodes
- hospitalization
- burnout
- or emotional instability during major life events
At this stage:
👉 the issue may still be highly manageable.
Stage 2 — Applicant Reacts Out of Fear
The applicant begins:
- hiding treatment
- stopping medication suddenly
- refusing counseling
- minimizing symptoms
- or emotionally overreacting to the process
This is where the danger often begins.
Because adjudicators may interpret these reactions as:
👉 unmanaged instability rather than responsible treatment management.
Stage 3 — The Record Becomes Unstable
The applicant:
- changes explanations repeatedly
- submits contradictory records
- refuses evaluations
- or creates inconsistent treatment narratives
Now the file begins feeling:
👉 difficult to assess and professionally unpredictable.
Stage 4 — Behavioral or Professional Problems Escalate
Additional concerns appear.
Examples may include:
- workplace issues
- emotional volatility
- impaired judgment
- treatment noncompliance
- or recurring emotional crises
At this point, adjudicators often begin viewing the issue as:
👉 unresolved future reliability risk.
Stage 5 — Credibility Problems Develop
The applicant:
- conceals treatment
- minimizes instability
- provides unsupported self-assessment
- or becomes emotionally reactive during investigation
Now the case may evolve into:
👉 a broader Guideline E credibility problem.
This is one of the most important realities of Guideline I:
👉 instability plus credibility concerns becomes much harder to mitigate than treatment alone.
Stage 6 — The Entire File Becomes a Predictability Concern
At this point, adjudicators begin questioning:
- judgment
- emotional control
- treatment reliability
- behavioral predictability
- and future stability
This is where many Guideline I cases ultimately fail.
Stage 7 — SOR or Denial
The unresolved psychological-condition concern hardens into:
- an LOI
- a Statement of Reasons
- suspension
- denial
- or revocation
👉 Final outcome: clearance loss.
How Guideline I Interacts With Other Guidelines
Guideline I frequently overlaps with several other security-clearance guidelines.
This is one reason psychological-condition cases can become much more complicated than applicants initially expect.
Many cases that begin as:
👉 emotional-stability concerns
eventually become:
👉 broader credibility, judgment, or behavioral-control cases.
Guideline E — Personal Conduct
This is one of the most common overlaps.
Examples include:
- concealing treatment
- minimizing instability
- inconsistent disclosures
- emotionally reactive explanations
- or contradictory statements during investigation
In many cases:
👉 the concealment becomes more dangerous than the underlying condition itself.
See:
👉 Guideline E — Personal Conduct
Guideline G — Alcohol Consumption
Psychological-condition concerns frequently overlap with:
👉 alcohol-related behavioral concerns.
Especially where alcohol appears connected to:
- emotional instability
- impulsive behavior
- depression
- PTSD
- or behavioral-control problems
See:
👉 Guideline G — Alcohol Consumption
Guideline H — Drug Involvement and Substance Misuse
Psychological-condition concerns sometimes overlap with:
👉 substance-use concerns.
Especially where applicants:
- self-medicate
- misuse prescriptions
- combine substances
- or demonstrate dependency-related behavior
See:
👉 Guideline H — Drug Involvement and Substance Misuse
Guideline J — Criminal Conduct
Some Guideline I cases overlap with:
👉 criminal-conduct concerns.
Especially where emotional instability contributes to:
- impulsive behavior
- arrests
- domestic incidents
- threats
- or emotionally driven misconduct
See:
👉 Guideline J — Criminal Conduct
Guideline F — Financial Considerations
Psychological instability sometimes contributes to:
👉 financial problems.
Examples may include:
- impulsive spending
- job instability
- debt
- gambling
- or inability to manage obligations during periods of emotional crisis
See:
👉 Guideline F — Financial Considerations
👉 Once multiple guidelines begin overlapping, the mitigation burden often becomes much heavier.
This is one reason early strategic handling matters enormously.
How Guideline I Appears Throughout the Clearance Process
Psychological-condition concerns can emerge at nearly every stage of the security-clearance process.
Many applicants mistakenly assume:
👉 “If I explain the issue once, it disappears.”
That is not how the system works.
Guideline I concerns often follow applicants throughout:
- the SF-86 process
- treatment disclosures
- background investigations
- subject interviews
- psychological evaluations
- medication review
- LOIs
- SORs
- hearings
- and future reinvestigations
This is why:
👉 early stabilization of the record matters enormously.
The SF-86 Stage
Many Guideline I cases first appear during completion of the:
👉 SF-86 Security Clearance Form
This is where applicants disclose:
- counseling
- therapy
- medication
- hospitalization
- emotional treatment
- and other mental-health-related information
The SF-86 becomes:
👉 the foundation of the psychological-condition investigative record.
If disclosures are:
- incomplete
- vague
- inconsistent
- or emotionally reactive
those problems often follow the applicant throughout the clearance process.
The Evaluation and Treatment Stage
Some Guideline I cases involve:
- psychological evaluations
- psychiatric records
- counseling history
- medication review
- hospitalization records
- or treatment recommendations
Adjudicators often evaluate:
- whether treatment was followed
- whether stability improved
- whether relapse or escalation occurred
- and whether current functioning appears reliable
This is one reason professional documentation matters enormously in Guideline I cases.
The LOI and SOR Stages
If psychological-condition concerns remain unresolved, applicants may receive:
At this stage, the government is often attempting to:
- clarify treatment history
- assess current stability
- evaluate future predictability
- and determine whether the issue is escalating
Poorly handled responses often become:
👉 the blueprint for later denial.
Related Guideline I Resources
For deeper analysis of the most common Guideline I issues, review:
👉 Can Prescription Drugs Affect a Security Clearance?
👉 How to Mitigate a Guideline I Psychological Conditions Security Clearance Concern
👉 The Whole Person Concept Explained: Why “Good People” Still Lose Clearance Cases
👉 How Security Clearance Risk Is Evaluated (What Actually Matters Most)
👉 What “Clearly Consistent with National Security” Really Means
How Guideline I Psychological Conditions Are Actually Mitigated
Many applicants assume that once mental-health-related concerns appear in the clearance process, the case is effectively over.
That is not true.
In reality, many Guideline I cases are highly mitigable when the issue is handled strategically and the record is stabilized correctly.
The key is understanding what adjudicators are actually evaluating:
👉 stability
👉 predictability
👉 treatment compliance
👉 professional functioning
👉 emotional control
👉 and whether future impairment risk appears manageable
Strong mitigation often involves:
- treatment compliance
- stable evaluations
- counseling participation
- medication management
- no recurring crises
- strong professional functioning
- and long-term behavioral predictability
For a deeper breakdown of what actually helps—and hurts—Guideline I cases, including therapy, PTSD, medication, hospitalization, emotional crises, and psychological-evaluation strategy, review:
👉 How to Mitigate a Guideline I Psychological Conditions Security Clearance Concern
The Record Controls the Case.
SECURITY CLEARANCE DENIED OR REVOKED
If you are appealing a security clearance determination, it is imperative that you obtain experienced legal representation. Doing so will provide you with the best opportunity to obtain or maintain your clearance.
Click Here For a No Obligation, Always Confidential Consultation